
Every Wednesday I work at my friend’s outpatient clinic as a part-timer psychiatrist. I am a medical doctor only for four hours a week. For the rest of time, I am a teacher of Individual Psychology.
At the clinic I do not only employ psychotherapy, but also prescribe medical drugs. I use Chinese herbal medicines together with modern chemical drugs. As a result, I can reduce doses of the chemical medicines. My father was a private practitioner, and he also liked the Chinese medicines. He often said, “I would not know how to treat some patients, if I did not learn the Chinese medical science.” I learned the traditional medicine from him, since we could not learn it at medical school. The Chinese medicines, for example, are very effective to emotional instability caused by menopausal disorders. Western drugs for the symptom often have strong side effects, but Chinese herbs are very mild with good results.
However, my patients are not so many. The reason is, perhaps, because they wish to be removed their symptoms in a short term. Both psychotherapy and Chinese medical treatment take time. Patients may be dissatisfied with it. They expect quick symptom removal; not long-term radical treatment. A good doctor is not necessarily a popular doctor.
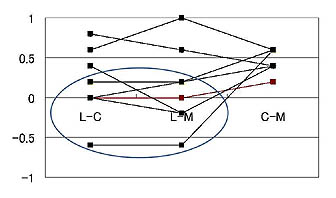
Am I really a good doctor? Of course I believe I am a good doctor by myself, but this may not be true. The graph in the right is from a study of my student[1]. It is about satisfaction of group counseling. She interviewed participants of group therapy sessions and asked some questions according to a fixed format. Then she examined the correlation between satisfaction of group leaders,(L) clients(C) who presented their own problems, and other members(M). L-C means the correlation between leaders and clients, L-M means it between leaders and members, and C-M means it between clients and members. The correlations between clients and members (C-M) are generally positive. Namely, when a client of a group was satisfied by a session, the members of the same group also are satisfied, and vice versa. However, the correlations between some leaders and their clients (L-C) and between leaders and their members (L-M), which are circled, are negative or almost zero. Namely, when a leader of a group is satisfied by a session, the client or the members of the same group may not be satisfied. Therefore, even if I am satisfied with my treatment, my patients may not be contended. In this case, can I say I am a good doctor?
Since Individual Psychology was introduced in Japan, a quarter of a century has passed. In recent several years, I encourage people to do such objective studies. Many interesting findings come out, and I want to introduce some of them at the International Congress of Individual Psychology. Last year, two of my colleagues presented interesting reports at Vilnius, Lithuania [2][3]. In the next Congress at Vienna, I hope Japanese researchers present much more papers.
[1] Haruka Miyamoto: The Impressions of Leaders and Members of Group Therapy Sessions. The Adlerian, 22(2), 2009. (Japanese)
[2] Ayako Ihara, Masako Seino, Shunsaku J. Noda: The Counseling Process in Parent-Study Groups based on Individual Psychology. The 24th International Congress of Individual Psychology, Vilnius, Lithuania, 2008.
[3] Hironori Nakajima, Tadashi Tanaka, Masako Hagi, Keiko Okada, Shunsaku J. Noda: Using Number One Priority and Sensory Types to Understand Life Style in the Group Workshop. The 24th International Congress of Individual Psychology, Vilnius, Lithuania, 2008.